Carried by: FIRENDO
References:
Clinician(s): Pr Jérôme BERTHERAT, Pr Pascal BARAT
Biologist(s): Pr Eric PASMANT, Dr. Florence ROUCHER-BOULEZ
Presentation
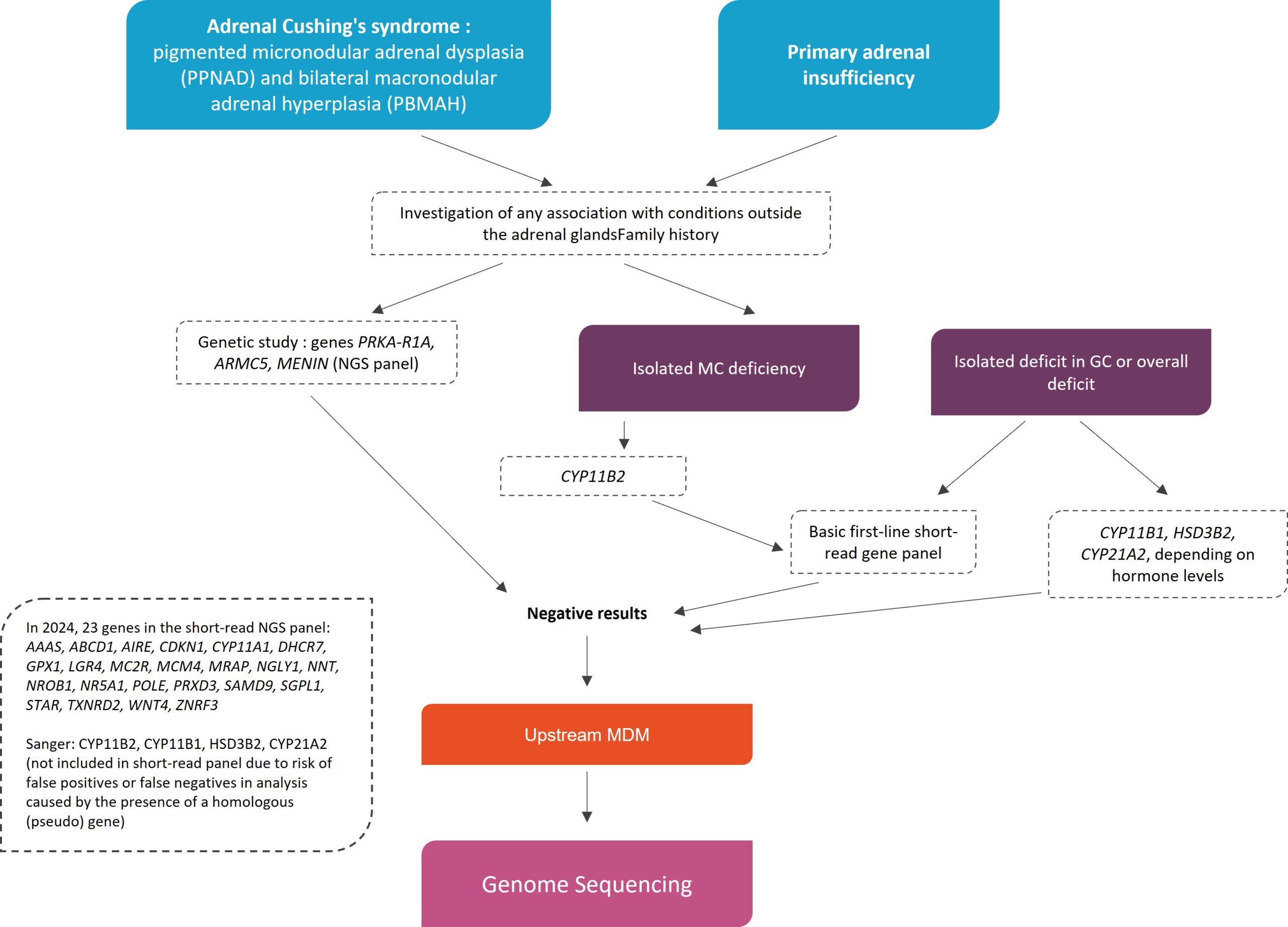
Bilateral nodular adrenal hyperplasia is a rare cause of Cushing’s syndrome (excessive secretion of adrenal steroids). It includes two diagnostic categories: pigmented micronodular adrenal dysplasia (PPNAD) and bilateral macronodular adrenal hyperplasia (PBMAH).
Congenital primary adrenal insufficiency, a life-threatening condition, is linked to a deficiency in steroid hormones due to adrenal cortex dysfunction. Symptoms appear in the first few months of life, sometimes during childhood, and can be more or less specific: hypoglycaemia, salt loss, dehydration.
Criteria before considering a discussion in MDM-FMG
Cushing’s syndrome due to bilateral nodular adrenal hyperplasia:
- Diagnostic criteria and hormonal and imaging investigations are detailed in the National Diagnostic and Care Programme (PNDS) for Cushing’s syndrome
- Biologically proven ACTH-independent Cushing’s syndrome (CLU, midnight F, DXM suppression test, baseline ACTH and/or after CRH)
- If patient has undergone surgery: confirmation of histological diagnosis of PPNAD or PBMAH
- If patient has not undergone surgery: adrenal imaging reviewed in a multidisciplinary team meeting to obtain expert agreement on the diagnosis of Cushing’s syndrome due to bilateral adrenal involvement
- Genetic testing for PRKAR1A, ARMC5, PRKACA, MENIN (NGS panel)
Primary Adrenal Insufficiency:
- Characterisation of PAI:
- Age at diagnosis, family history and consanguinity, associated extra-adrenal manifestations
- In all patients: Na+, K+, ACTH, renin, cortisol, DHEAS, 17OH-Progesterone, (FSH, LH, T, E2, adrenal ultrasound)
- In all boys >3 years of age: very long chain fatty acids
- In cases of suspected autoimmune disease and depending on age: anti-adrenal or anti-21OH antibodies
- (In girls or 46XY with DSD: karyotype if ultrasound does not confirm normal ovaries and Müllerian structures, AMH)
- Inconclusive analysis of first-line genes:
- In 2024: 23 genes in a short read panel ideally containing SRY to highlight phenotypic-chromosomal sex discordance: AAAS ABCD1 AIRE CDKN1C CYP11A1 DHCR7 GPX1 LGR4 MC2R MCM4 MRAP NGLY1 NNT NR0B1 NR5A1 POLE PRDX3 SAMD9 SGPL1 STAR TXNRD2 WNT4 ZNRF3
- Sanger: CYP11B2, CYP11B1, HSD3B2, CYP21A2 if hormonal test suggest such an enzyme block
Genome Sequencing in diagnostic strategy
MDM cartography
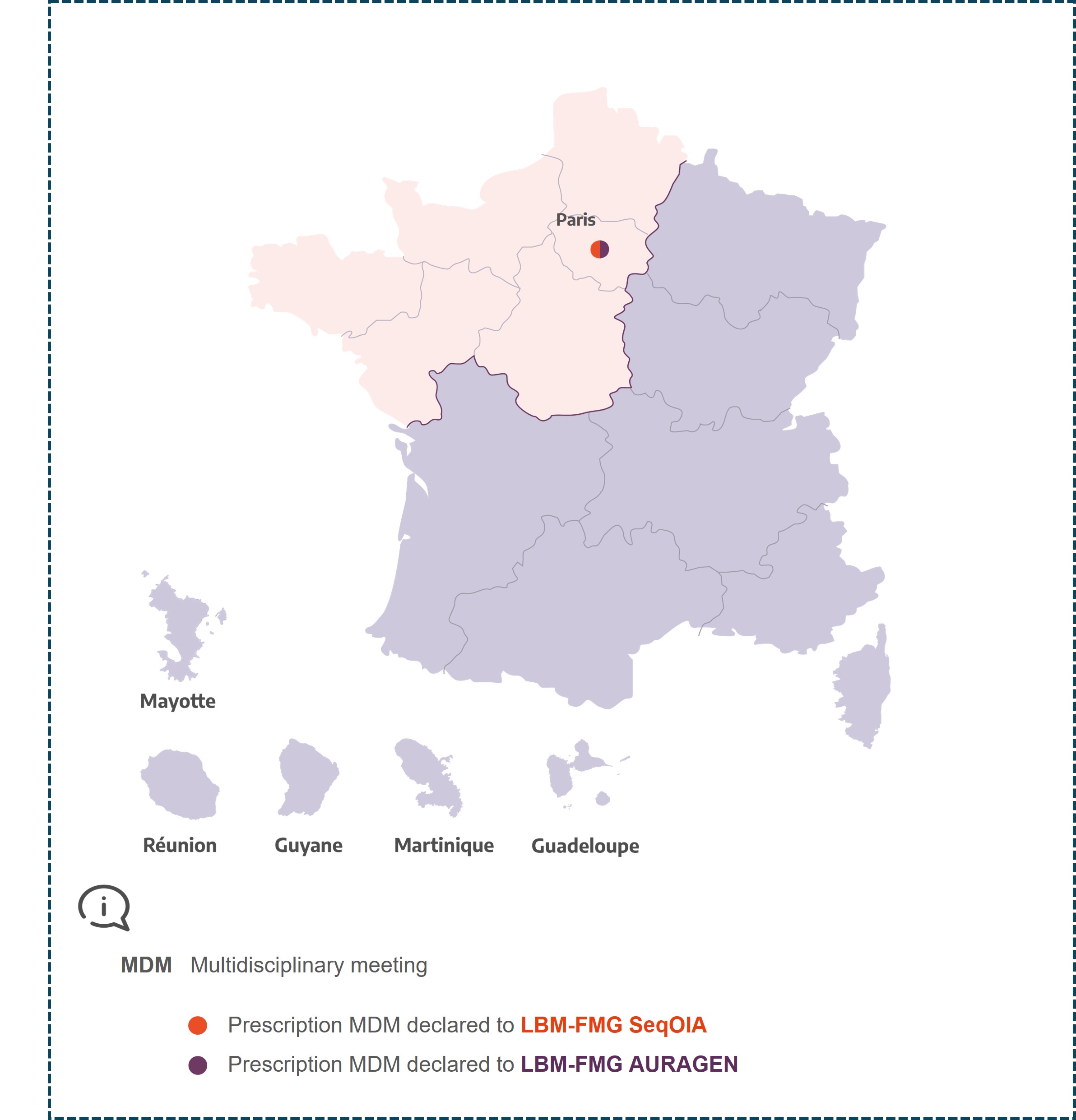
MDM
Type of the MDM
City of the coordinator
Name, first name, and email of the contact